✅ What you’ll learn from this article
💡 Accurate knowledge about sebaceous cysts
💡 A clear understanding of the difference from epidermoid cysts
💡 Available treatment options to help ease your concerns
⚠️ If left untreated
❌ The number of cysts may continue to increase
❌ Inflammation can develop, causing pain
❌ In rare cases, it may be a sign of a more serious condition
At IC Clinic Ueno, we provide accurate diagnosis and appropriate treatment for sebaceous cysts. We are committed to understanding each patient’s individual concerns and ensuring you can receive care with confidence and peace of mind.
😟 “I have several small bumps on my chest and neck that bother me.”
😰 “There was just one at first, but it seems like more keep appearing.”
😱 “What condition could this be? Could it spread to other people?“
Do any of these concerns sound familiar?
If you have multiple small, pale yellow or skin-colored raised bumps on your chest, neck, or underarms, you may be experiencing a skin condition called sebaceous cysts (steatocystoma).
Sebaceous cysts are benign skin lesions that are not uncommon, yet they are frequently confused with epidermoid cysts and similar conditions, leaving many people without accurate knowledge. Because they often appear in multiples, it is also understandable to worry about whether they will keep increasing in number.
On this page, we explain sebaceous cysts in detail and offer a clear overview of the available treatment options.
🔍 What Are Sebaceous Cysts?
Sebaceous cysts are benign cystic tumors that arise from the sebaceous glands, which secrete sebum [1,2]. Formally referred to as “sebaceous cysts” (sebaceous cyst), they are classified as a type of cutaneous adnexal tumor [1,11]. Sebaceous cysts are a relatively rare skin condition, estimated to account for approximately 1–2% of all skin tumors [2,14].
Solitary sebaceous cysts occur sporadically, whereas multiple cysts are strongly associated with hereditary conditions [4,5,7]. In particular, hereditary tumor syndromes such as Muir-Torre syndrome are known to present with multiple sebaceous tumors as a characteristic skin manifestation [4,5,9,10].
📊 Epidemiology and Incidence of Sebaceous Cysts
Sebaceous cysts are a relatively rare condition, with an estimated annual incidence of approximately 0.5–1 case per 100,000 people [2,14]. There is little difference in incidence between males and females, and while the age of onset spans a wide range, they are more commonly seen in adults [1,2].
📍 Preferred sites include areas with abundant sebaceous glands:
- 💛 Anterior chest (approximately 40%)
- 💛 Axillae (approximately 25%)
- 💛 Neck (approximately 20%)
They can also occur on the face and scalp, though at these sites, secondary development from nevus sebaceus should also be considered [15,17].
🧬 Genetics and Molecular Biology of Sebaceous Cysts
Solitary sebaceous cysts are generally sporadic, whereas genetic factors play an important role in multiple sebaceous cysts [7]. Mutations in the keratin 17 (K17) gene, which follows an autosomal dominant inheritance pattern, have been reported; these mutations are thought to result in abnormal differentiation of sebaceous glands [7].
In Muir-Torre syndrome, mutations in DNA mismatch repair genes (MSH2, MLH1, MSH6, PMS2) characteristically lead to a combination of sebaceous tumors and visceral malignancies—particularly colorectal cancer [4,5,9,10]. In this syndrome, sebaceous tumors, including sebaceous cysts, serve as important cutaneous warning signs [5,13].
🔬 Histopathological Features and Diagnosis
The histopathological features of sebaceous cysts include a cyst wall composed of mature sebaceous cells and sebum-like contents within the cavity [2,12]. Immunohistochemically, sebaceous markers such as adipophilin and perilipin-1 are positive, which is useful for confirming the diagnosis [2,12].
✨ Here’s how to tell them apart from epidermoid cysts!
The most important differential diagnosis is distinguishing sebaceous cysts from epidermoid cysts (atheroma) [1,3].
- ❌ Epidermoid cysts: a central punctum (navel-like opening) is present
- ⭕ Sebaceous cysts: no central punctum
- ⭕ Sebaceous cysts: tend to occur in multiples
💡 Causes of Sebaceous Cysts
Sebaceous cysts are thought to develop due to obstruction of the opening or duct of a sebaceous gland—the gland responsible for secreting sebum onto the skin surface [1,2].
🔹 Solitary cases
A non-hereditary cause is common, with secondary ductal obstruction resulting from trauma or inflammation often implicated [1].
🔹 Multiple cases
Genetic factors play an important role, and mutations in the keratin 17 (K17) gene following an autosomal dominant inheritance pattern have been reported [7]. These gene mutations are thought to cause abnormal differentiation of the pilosebaceous unit, resulting in the development of multiple sebaceous cysts [7].
Sebaceous cysts can also develop secondarily from nevus sebaceus [15,17]. In such cases, hormonal changes after puberty may activate the nevus sebaceus, potentially giving rise to various sebaceous tumors (sebaceous cysts, sebaceous adenomas, sebaceous carcinomas, etc.) [15,17].
😷 Symptoms of Sebaceous Cysts
Sebaceous cysts most commonly appear on the anterior chest, axillae, and neck—areas with abundant sebaceous glands [1,14]. They present as skin-colored or pale yellow, hemispherical, elevated nodules with a smooth surface and are freely movable [1,2].
⚠️ The most characteristic feature of sebaceous cysts
Cluster formation: multiple cysts tend to develop in close proximity [14]. Although solitary cysts do occur, new cysts often appear in the surrounding area over time [14].
Sebaceous cysts are generally asymptomatic, but if the cyst wall ruptures and inflammation develops, swelling and pain may occur [1,3]. Rupture of the cyst can cause sebum-like contents to leak into surrounding tissue, sometimes leading to the formation of inflammatory granulation tissue [1].
🔍 Key distinguishing features from epidermoid cysts (atheroma):
- ✅ Sebaceous cysts do not show a central punctum [1]
- ✅ Their tendency to occur in multiples is also a useful finding for differentiation [14]
🩺 Diagnosis and Examination of Sebaceous Cysts
The diagnosis of sebaceous cysts is primarily based on clinical features [1,11]. Visual examination reveals hemispherical nodules ranging from skin-colored to pale yellow, while palpation shows soft, elastic, and freely movable lesions [1].
📋 Imaging examinations
- 🔹 Ultrasound: depicts the lesion as a cystic structure with a homogeneous hypoechoic area [16]
- 🔹 MRI: high signal intensity on T1-weighted images—comparable to fat—and high signal on T2-weighted images as well [16]
Definitive diagnosis requires histopathological examination, with confirmation of a cyst wall composed of mature sebaceous cells being essential [2,12]. Immunohistochemical testing shows positive results for sebaceous markers such as adipophilin and perilipin-1 [2,12].
⚠️ Important note for multiple sebaceous cysts!
The possibility of hereditary tumor syndromes such as Muir-Torre syndrome should be considered, and it is advisable to obtain a thorough family history and discuss genetic testing [4,5,13].
💊 Treatment of Sebaceous Cysts
The definitive treatment for sebaceous cysts is surgical excision [3,16]. Complete removal, including the cyst wall, can help reduce the risk of recurrence [3,16]. Surgery is performed under local anesthesia, and the incision line is determined based on the size and location of the cyst [16].
⚠️ Aspiration alone may lead to recurrence!
Drainage by needle aspiration provides temporary reduction, but since the cyst wall remains, recurrence is common [3]. Therefore, even when the goal is symptomatic relief, surgical excision is ultimately recommended [3,16].
🔹 Multiple sebaceous cysts
Treatment decisions are made by comprehensively weighing aesthetic and functional considerations [14]. Since removing all cysts at once is not always practical, treatment is often carried out in stages according to the patient’s preferences and the severity of symptoms [14].
🔹 Carbon dioxide (CO2) laser treatment
This is another option; however, since complete removal of deep cyst walls may not always be achievable, the risk of recurrence must be carefully considered when determining its suitability [16].
📈 Post-Treatment Course and Prognosis
✨ With appropriate treatment, the prognosis is favorable!
With appropriate surgical excision, the prognosis is generally favorable, and the recurrence rate following complete removal has been reported to be below 5% [3,16]. Post-operative complications are uncommon and are generally limited to temporary swelling and mild discomfort [16].
⚠️ For multiple sebaceous cysts associated with hereditary conditions such as Muir-Torre syndrome, regular dermatological follow-up and internal medicine screening (including colorectal cancer screening) are important [4,5,13].
⚠️ Complications and Precautions Regarding Sebaceous Cysts
The primary complication of sebaceous cysts is inflammation resulting from rupture of the cyst wall [1,3]. Rupture allows sebum-like contents to leak into surrounding tissue, triggering a foreign-body inflammatory reaction [1].
🚨 Multiple sebaceous cysts require careful attention!
The possibility of hereditary tumor syndromes, including Muir-Torre syndrome, should always be kept in mind [4,5,13]. In this syndrome, sebaceous tumors may present as a warning sign of colorectal or genitourinary cancers, making early detection and early intervention critically important [5,10].
For sebaceous cysts associated with nevus sebaceus, there is a risk of malignant transformation (sebaceous carcinoma) after puberty, and regular monitoring is necessary [15,17,18]. If rapid growth or ulceration is observed, a tissue biopsy should be performed promptly [17,18].
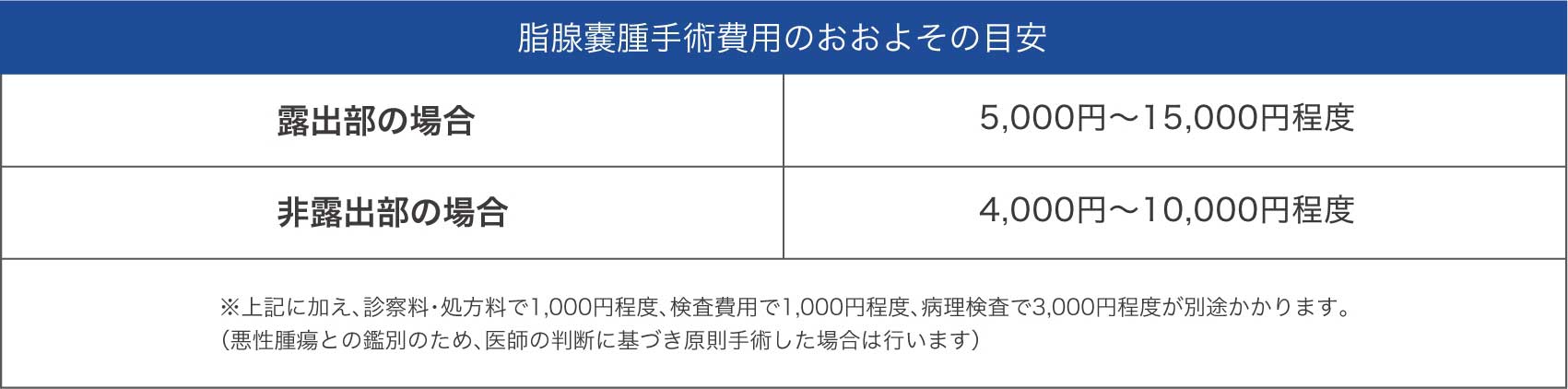
💰 Cost of Sebaceous Cyst Surgery
❓ Frequently Asked Questions About Sebaceous Cysts
Q1: Do sebaceous cysts resolve on their own?
💬 A: Sebaceous cysts rarely resolve on their own [1,3]. As long as the cyst wall remains, the contents will re-accumulate and the cyst will recur [3]. Surgical excision is required for definitive treatment [3,16].
Q2: What is the difference between a sebaceous cyst and an epidermoid cyst (atheroma)?
💬 A: The most important distinction is that epidermoid cysts typically show a central punctum (navel-like opening), whereas sebaceous cysts do not [1]. Additionally, sebaceous cysts tend to occur in multiples, which is also a helpful clue for differentiation [14].
Q3: Could multiple sebaceous cysts indicate a hereditary condition?
💬 A: Multiple sebaceous cysts may be associated with hereditary tumor syndromes such as Muir-Torre syndrome [4,5]. As this can carry an elevated risk of visceral malignancies such as colorectal cancer, genetic counseling and genetic testing are worth discussing with a specialist [5,13].
Q4: What is the recurrence rate after surgery?
💬 A: When complete excision including the cyst wall is performed, the recurrence rate is reported to be below 5%, indicating a favorable outcome [3,16]. However, incomplete excision or aspiration alone carries a higher likelihood of recurrence, which is why appropriate surgical treatment is important [3].
🏥 At IC Clinic Ueno
✅ Accurate diagnosis by experienced specialist physicians
✅ Careful complete excision to help reduce the risk of recurrence
✅ Same-day treatment under local anesthesia
✅ Cosmetically considerate care with attention to post-operative scarring
📚 References
- Japanese Dermatological Association, ed. Dermatology, 11th Edition. Bunkodo, 2018.
- Fernandez-Flores A, Saeb-Lima M, Cassarino DS. Histopathology of sebaceous neoplasms. Am J Dermatopathol. 2009;31(5):440-451.
- Zuuren EJ, Fedorowicz Z, Arents BWM. Interventions for sebaceous cysts. Cochrane Database Syst Rev. 2014;(12):CD007951.
- Ponti G, Luppi G, Losi L, et al. Muir-Torre syndrome and MSH2 gene alterations: a not uncommon association in hereditary nonpolyposis colorectal cancer families. Hum Mutat. 2005;26(6):546-553.
- Schwartz RA, Torre DP. The Muir-Torre syndrome: a 25-year retrospect. J Am Acad Dermatol. 1995;33(1):90-104.
- Japanese Society of Plastic and Reconstructive Surgery, ed. Plastic and Reconstructive Surgery, 4th Edition. Kokuseido, 2017.
- Lisle A, Mosier M, Kandamany N. Multiple sebaceous cysts and the keratin 17 gene mutation: a case report. Dermatol Online J. 2008;14(1):7.
- Harii K, Hashimoto K, eds. NEW Dermatology, 3rd Edition. Nakayama Shoten, 2018.
- Smith KJ, Skelton HG 3rd, Lupton GP, et al. Sebaceous carcinoma and the Muir-Torre syndrome. J Cutan Pathol. 1995;22(4):378-385.
- Akhtar S, Oza KK, Khan SA, Wright J. Muir-Torre syndrome: case report of a patient with concurrent jejunal and ureteral cancer and a review of the literature. J Am Acad Dermatol. 1999;41(5 Pt 1):681-686.
- Japanese Dermatological Association. “Clinical Practice Guidelines for Skin Tumors, 2nd Edition,” 2015.
- Bowen AR, LeBoit PE. Sebaceous neoplasms of the skin. Am J Dermatopathol. 2005;27(4):315-326.
- Shalin SC, Lyle S, Calonje E, Lazar AJ. Sebaceous neoplasia and the Muir-Torre syndrome. Pathology. 2010;42(3):223-230.
- Editorial Committee of the Japanese Journal of Dermatology. “Diagnosis and Treatment of Sebaceous Cysts.” Jpn J Dermatol. 2017;127(3):543-558.
- Kossard S, Epstein EH Jr, Cerio R, et al. Basal cell carcinoma and sebaceous hyperplasia in nevus sebaceus: a morphologic study of 99 cases. J Am Acad Dermatol. 1994;30(3):373-378.
- Robinson JK, Hanke CW, Siegel DM, et al. Surgery of the Skin: Procedural Dermatology, 3rd Edition. Elsevier, 2015.
- Kazakov DV, Kutzner H, Rutten A, et al. Carcinomas arising in preexisting sebaceous nevus: a clinicopathologic study of 75 cases. Am J Surg Pathol. 2007;31(11):1628-1636.
- Miller CJ, Ioffreda MD, Billingsley EM. Sebaceous carcinoma, ocular adnexa: a review of 14 cases. Dermatol Surg. 2001;27(1):93-96.
- Harvey RG, Harman KE, Morris SD. Multiple steatocystomas and hidrocystomas: the complete spectrum of sebaceous differentiation in organoid naevi. Br J Dermatol. 2001;144(4):886-890.
- Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors, 6th Edition. Elsevier, 2014.